Hello Dyinshadows,
Congratulations on overcoming some of the symptoms of Aspergers!
You certainly sound like an intelligent young person! Many Aspies are
highly intelligent!
What Risperdal ?does?, all comes down to brain chemistry! Risperdal
does not work on everyone, and is actually not totally understood!
?Attention deficit hyperactivity disorder (ADHD) is one of a number
of behavioural and developmental disorders that affect young children.
A child with ADHD has three main behavioural issues: inattention,
impulsivity and overactivity. All young children have a limited
attention span and sometimes do things without thinking. Only a few of
these children have ADHD. Treatment for ADHD is complex and may
include drug therapy, behavioural management, psychological
counselling and family support groups. Treatment using medication is
fast and - in many cases - effective, but research suggests that using
a multifaceted approach ensures a greater success rate.
Drugs target the brain's neurotransmitters
Neurotransmitters are brain chemicals. There is some evidence to
suggest that genetic abnormalities may prevent the child with ADHD
from metabolising key neurotransmitters in normal ways. However, no
specific brain defect has been found that could account for ADHD,
which also means there is probably no single drug that can correct the
problem.?
http://www.disability.vic.gov.au/dsonline/dsarticles.nsf/pages/Attention_deficit_hyperactivity_disorder_-_drug_therapy?OpenDocument
Risperidone is one of several atypical neuroleptics, also known as
atypical antipsychotics.
Simply put: ?Risperidone is an antipsychotic medication that works
by interfering with the communication among nerves in the brain. The
nerves communicate with one another by producing and releasing
chemicals called neurotransmitters. The neurotransmitters attach to
receptors on other nearby nerves, and the attachment of the
neurotransmitter causes changes in the cells that have the receptor on
them. Risperidone blocks several of the receptors on nerves including
dopamine type 2, serotonin type 2, and alpha 2 adrenergic receptors
and this blocks communication among nerves. Risperidone is a
relatively new antipsychotic medication that probably has fewer side
effects than many of the older medications.?
http://www.answers.com/topic/risperidone
To completely understand how Risperidone works in the brain, you?ll
need to understand neurotransmitters:
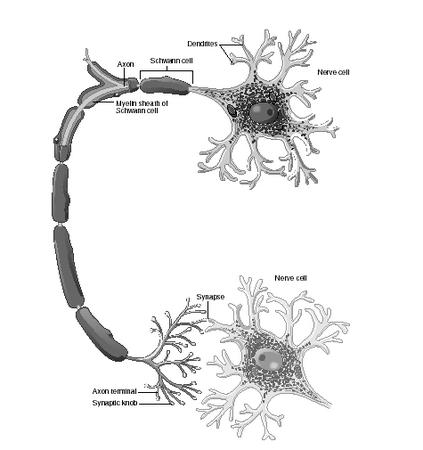
?Neurotransmitters are chemicals used to transmit messages in the
brain. Nerve cells have dendrites at one end and an axon (a long
tail-like thing) at the other. Axons communicate with dendrites at
synapses, the spaces between nerve cells. Electrical impulses travel
down the axon of a nerve cell to the synapse; when they get there,
they cause neurotransmitters to be released. The neurotransmitters
bind to receptors on the dendrite of the other cell in the synapse.
Different neurotransmitter receptors affect different bodily
functions. Serotonin, for example, has as many as seven receptor
types, and one of those has five subtypes. These receptors are
involved in regulating emotion, mood, impulsivity, aggression,
digestion, smooth muscle relaxation, and sexual behavior, among other
functions.
Three sorts of neurotransmitters have been of concern to scientists
studying self-injurious behavior: serotonin, dopamine, and endorphins.
The strongest evidence so far points to serotonergic deficits -- the
brain does not have enough serotonin available for use.?
?Risperidone, another relatively new neuroleptic, binds D2 dopamine
and 5-HT2 serotonin receptors; it has been reported by Khouzam and
Donnelly (1997) to reduce SIB in a patient with borderline personality
disorder. Olanzapine (Zyprexa) is another atypical neuroleptic used by
some psychiatrists to treat SIB. There are no well-controlled studies
of these drugs, however; the literature on them consists mainly of
case reports and again, no one has made a distinction between types of
SIB. These drugs can also have troublesome side effects -- patients on
clozapine, for example, require weekly blood tests because of the risk
of white-blood-cell abnormalities.?
http://www.palace.net/llama/psych/pharm.html
?The picture became easier to understand when chemicals in the brain
called "neurotransmitters" were discovered. The brain consists of
billions of neurons or cells that must communicate with each other.
The communication between neurons maintains all body functions,
informs us when a fly lands on our hand, or when we have pain. The
communication between neurons is controlled by the brain's type and
level of neurotransmitters. Neurotransmitters are chemical substances
that control and create signals in the brain both between and within
neurons.
Without neurotransmitters, there would be no communication between
neurons. The heart wouldn't get a signal to beat, arms and legs
wouldn't know to move, etc.
As we discovered more about neurotransmitters, we began to identify
which neurotransmitters controlled certain bodily functions or which
were related to certain emotional/psychiatric difficulties. Serotonin,
a neurotransmitter, was found to be related to body temperature and
the onset of sleep. Research also identified Serotonin as related to
depression and later to a variety of mental health conditions such as
anorexia and obsessive-compulsive disorder.
As research in neurotransmitters continued, studies between
neurotransmitters and mental conditions revealed a strong connection
between amounts of certain neurotransmitters in the brain and the
presence of specific psychiatric conditions. Using an everyday
example, our automobile operates by using a variety of fluids such as
engine oil, transmission fluid, brake fluid, and coolant
(anti-freeze). Every automobile has a way to measure the levels or
amounts of each of these needed liquids such as the dipstick for oil
and transmission fluid and marked indicators for anti-freeze and
brake-fluid levels. Using our dipstick to measure engine oil, for an
example, we can find our engine to be found one, two, or even three
quarts low. After a recent oil change, the dipstick may also tell us
that we have excessive oil in the engine.
To work properly, all fluid levels must be in the "normal range" as
indicated by the dipstick. When we receive a blood test, values of
certain blood components are given with the "normal range" also
provided, indicating if a blood chemical is below or above the average
range.
Neurological research has identified over fifty (50) neurotransmitters
in the brain. Research also tells us that several neurotransmitters
are related to mental health problems ? Dopamine, Serotonin,
Norepinephrine, and GABA (Gamma Aminobutyric Acid). Too much or too
little of these neurotransmitters are now felt to produce psychiatric
conditions such as schizophrenia, depression, bi-polar disorder,
obsessive-compulsive disorder, and ADHD.?
?Serotonin, first isolated in 1933, is the neurotransmitter that has
been identified in multiple psychiatric disorders including
depression, obsessive-compulsive disorder, anorexia, bulimia, body
dysmorphic disorder (nose doesn't look perfect after ten surgeries),
social anxiety, phobias, etc. Serotonin is a major regulator and is
involved in bodily processes such as sleep, libido (sexual interest),
body temperature, and other areas.
Perhaps the best way to think of Serotonin is again with an automobile
example. Most automobiles in the United States are made to cruise at
70 miles per hour, perfect for interstate highways and that summer
vacation. If we place that same automobile on a racetrack and drive
day-after-day at 130 mph, two things would happen. Parts would fail
and we would run the engine so hot as to evaporate or burnout the oil.
Serotonin is the brain's "oil".
Like a normal automobile on a race track, when we find ourselves
living in a high stress situation for a prolonged period of time, we
use more Serotonin than is normally replaced. Imagine a list of your
pressures, responsibilities, difficulties and environmental issues
(difficult job, bad marriage, poor housing, rough neighborhood, etc.).
Prolonged exposure to such a high level of stress gradually lowers our
Serotonin level. As we continue to "hang on" we develop symptoms of a
severe stress-produced depression.
An automobile can be one, two or three quarts low in oil. Using the
automobile as an example, imagine that brain Serotonin can have
similar stages, being low (one quart low), moderately low (two quarts
low), and severely low (three quarts low). The less Serotonin
available in the brain, the more severe our depression and related
symptoms.? Please read further on this page for great explanations of
neurotrnsmitters!
http://www.mental-health-matters.com/articles/article.php?artID=160
?The brain is mostly made up of two kinds of cells. The first kind,
neurons, do the hard work of transmitting all that information. The
second kind, glial cells, are twice as numerous as neurons. Glial
cells have the less glamorous jobs of making sure the neurons have
enough nutrients and other chemicals, repairing the brain if it is
injured, and confronting bacteria that try to attack the brain.
Obviously, problems with either type of cell could be involved in
PDDs, and if one type of cell is affected, that would change how the
other type functions as well.?
?Autopsy studies over the past twenty years have indicated some
differences at the cell level in people with autism. Neurons in the
limbic system of the brain seem to be smaller and closer together,
while neurons in other areas of the brain may be larger or smaller
than usual. There appears to be a loss of Purkinje cells (a particular
type of neuron) in the cerebellum. Some cell differences seem to
depend on the age of the person, with brains from autistic children
tending to be larger than normal and brains from autistic adults
smaller than usual.?
?Neurons are the brain's internal communication centers, but they
don't trade messages directly. Neurons have a central cell body with
long "arms" called axons, and smaller tentacle-like structures called
dendrites. Inside a neuron, all the messages are sent via electrical
impulses. Where two neurons meet to swap information, however, there's
a small space between them called the synaptic cleft. Electrical
impulses have to be translated into neurotransmitters, chemicals that
cross the synaptic cleft and are then re-translated into electrical
signals on the other side.
Much has been learned about the role of neurotransmitters in PDDs by
accident. For example, autistic symptoms improved in some patients
when they were taking medicines for something else, such as
depression. Now, targeted studies of medications indicate that several
kinds of neurotransmitters have something to do with PDDs.?
http://www.patientcenters.com/autism/news/neurology.html
Aytpical Antipsychotic medications have come around more recently and
have been used to help mental conditions such as:
*schizophrenia
*psychosis
*self-injurious behavior
*painful ticcing
*autism/PDD
These newer antipsychotics, the atypicals, have fewer side effects
than the original conventional antipsychotic medications.
http://www.angelfire.com/tn3/task/neuroleptics.html
A little more scientific explanation: ?Blockade of dopaminergic D2
receptors in the limbic system alleviates positive symptoms of
schizophrenia such as hallucinations, delusions, and erratic behavior
and speech. Blockade of serotonergic 5-HT2 receptors in the
mesocortical tract, causes an excess of dopamine and an increase in
dopamine transmission, resulting in an increase in dopamine
transmission and an elimination of core negative symptoms. Dopamine
receptors in the nigrostriatal pathway are not affected by risperidone
and extrapyramidal effects are avoided. Like other 5-HT2 antagonists,
risperidone also binds at alpha(1)-adrenergic receptors and, to a
lesser extent, at histamine H1 and alpha(2)-adrenergic receptors.?
http://redpoll.pharmacy.ualberta.ca/drugbank/cgi-bin/getCard.cgi?CARD=APRD00187.txt
?By blocking dopamine-2 receptors, haloperidol prevents the binding of
dopamine to its receptor in the synaptic cleft, which is the space
between brain cells (neurons) where neurotransmitters modulate
communication within the brain. Thus haloperidol stops the effects of
dopamine in the synaptic cleft and decreases dopaminergic transmission
between neurons.?
?Risperidone, as it effectively blocks dopamine-2 receptors, inhibits
the dopaminergic pathway projecting to the pituitary gland, and this
can affect the regulation of prolactin secretion. Prolactin induces
lactation and ovulation, and its release from the pituitary gland is
inhibited by dopamine. Risperidone, via the inhibition of dopamine,
can induce prolactin secretion and thus cause these side effects.
Fortunately, risperidone rarely causes these side effects and when it
does, the side effects resolve with discontinuation of the medication.
This was the case with this woman.?
http://www.mnsu.edu/comdis/isad8/papers/lavid8.html
?As yet, there are no pharmacologic interventions that specifically
target the core deficits of the PDD profile. However, some progress
has been made in ameliorating the behavioral symptoms associated with
PDD. A number of studies, published since the 1960s, have shown that
improved control of behavioral symptoms can be achieved through the
use of conventional neuroleptics such as the dopamine receptor
antagonist haloperidol.3,5 The frequent occurrence of dyskinesias and
other extrapyramidal side effects limited their use. Not surprising,
as the early safety and efficacy data with the newer atypical
antipsychotics became available in the late 1980s and early 1990s,
interest in their use in PDD began to grow.
Risperidone is an antagonist of both dopamine (D2) and serotonin
(5HT2A and others) receptors.6,7 Particularly when used at lower
doses, risperidone proved to be relatively free of the extrapyramidal
symptoms (EPSs) that had limited the use of conventional agents.8 A
number of open-label trials were undertaken to investigate the use of
risperidone in children with PDD.9?18 Preliminary evidence from these
studies suggested that risperidone was both safe and effective in
reducing behavioral symptoms in this population. However, more
rigorously designed studies were needed to confirm these findings. At
the time that this study was conducted, no controlled studies had been
reported. As a result, this study was undertaken to evaluate
critically the efficacy and safety of risperidone for the treatment of
behavioral symptoms in children with PDD.?
http://pediatrics.aappublications.org/cgi/content/full/114/5/e634
?Risperidone is well-tolerated and effective at treating behavioral
symptoms associated with pervasive developmental disorders (PDD) and
autism, according to the results of a randomized trial published in
the November issue of Pediatrics.
"As yet, there are no pharmacologic interventions that specifically
target the core deficits of the PDD profile," write Sarah Shea, MD,
from IWK Health Centre and Dalhousie University in Halifax, Nova
Scotia, Canada, and colleagues. "Risperidone is an antagonist of both
dopamine (D2) and serotonin (5HT2A and others) receptors. Particularly
when used at lower doses, risperidone proved to be relatively free of
the extrapyramidal symptoms (EPSs) that had limited the use of
conventional agents."
http://www.medscape.com/viewarticle/493059
?"Typically, ADHD is described as a chemical imbalance, but our
research has shown that there may also be subtle anatomical
differences in areas of the brain that are important in this
disorder," co-principal investigator Dr. Sanjiv Kumra, a psychiatrist
at the Zucker Hillside Hospital in Glen Oaks, N.Y., said in a prepared
statement.
"We found abnormality of the fiber pathways in the frontal cortex,
basal ganglia, brain stem and cerebellum," said study author Manzar
Ashtari, an associate professor of radiology and psychiatry at the
North Shore-Long Island Jewish Health System in Hyde Park, N.Y.
"These areas are involved in the processes that regulate attention,
impulsive behavior, motor activity and inhibition ? the key symptoms
in ADHD children. They are also known to be part of a bigger circuit
in the brain that establishes communication between the frontal lobe
and cerebellum," Ashtari said in a prepared statement.?
http://abcnews.go.com/Health/Healthology/story?id=290724
?Asperger's syndrome can sometimes appear to be like depression, and vice versa.
Asperger's syndrome can be mistaken for or written off as depression
by some people for several reasons. Firstly, people with Asperger's
syndrome are just as likely to suffer from depression as anyone else
amongst the population, and it is pretty common. Secondly, having
Asperger's syndrome can be pretty depressing sometimes, and things
like stress, social isolation, and bullying could also cause
depression. Thirdly, for reasons I doubt I will ever understand,
'normal' people have a habit of assuming that everyone experiences
life the same way as them, so if they don't see you doing the same
things that they do they assume you must be depressed.
Likewise, someone who doesn't have Asperger's syndrome but who has
depression would stop doing the things they normally do to have fun
and would find no pleasure in them. Depression doesn't exactly tend to
make you popular either so it could lead to problems in relationships
with other people. Depression though is an illness... it can be
treated and you can recover from it. You can usually identify when you
became depressed and when you ceased to be depressed, and during the
times when you were not depressed you won't have had any of the
problems that characterise Asperger's syndrome.?
http://www.as-if.org.uk/overlap.htm#Attention%20Deficit%20Hyperactivity%20Disorder%20(Adhd)
?Action, if known: Risperdal affects serotonin and dopamine, and
raises the level of the hormone prolactin.?
http://www.oreilly.com/medical/autism/news/med_reference.html
?Risperidone is a very strong dopamine blocker (antagonist); i.e., it
inhibits functioning of postsynaptic dopamine receptors.
It reaches peak plasma levels quickly regardless of whether it is
administered as a liquid or pills. The strong dopamine-blocking
reaction is known to make some people feel nauseated if they do things
that normally trigger the dopamine response, such as eat a pleasing
meal or experience orgasm. Risperidone is metabolised fairly quickly
so this potential for nausea subsides usually in two to three hours.?
http://en.wikipedia.org/wiki/Risperidone
The above page also has a nice illustration:
http://en.wikipedia.org/wiki/Image:Risperidone-icon.jpg
?There is, however, potentially a way to maximize the "enhancing"
properties of an antidepressant medication without significantly
increasing the incidence of agitation and the potential for rage
behaviour. One can combine a partial and selective post-synaptic 5HT2
serotonin antagonism of low-dose Risperdal (Risperidone) with the
overall presynaptic serotonin enhancing effect of an antidepressant
medication, for a significantly improved overall response. For
example, a SSRI, e.g. Prozac, Paxil, Zoloft, Luvox, etc. and Risperdal
will often work together synergistically for three reasons. The first
reason, is that by controlling the post-synaptic serotonin receptor
response (floodgate control) with a low-dose Risperdal, one can
effectively eliminate, or at least reduce the possibility of increased
agitation, rage and insomnia with the introduction of the SSRI.
The second reason, is that both Risperdal and the SSRI will compete
for the same Cytochrome P450 Microenzyme ~ IID6, thereby significantly
raising each other?s therapeutic blood levels. The third reason,
relates to the selective blocking of the pre-synaptic 5-HT serotonin
receptors and the downgrading of the post-synaptic 5-HT2 serotonin
receptors over time by the SSRI, further complementing the serotonin
antagonism (blocking action) by the Risperdal. We have observed that
at a clinical level, this beneficial synergistic action between
Risperdal and a SSRI, only holds true when there is clear-cut evidence
of a major depression axis component with associated elements of
anxiety and agitation. If this medication combination is used in a
client with an unstable atypical rapid cycling bipolar or a bipolar I
- manic mood modulation pattern, one will usually observe a very
significant worsening in the degree of agitation and rage behaviour.
In the few cases where a major depression exists without any elements
of free floating anxiety, panic or agitation (very unusual in the
Autistic/PDD population), the antidepressant medication should be used
on its own, since a post-synaptic serotonin block with Risperdal, may
worsen the depression. In practical terms, if an antidepressant
medication is being considered for an Autistic/PDD client, in most
cases, it would be advisable to have in place a partial post-synaptic
serotonin receptor block with 0.5 to 1.5 mg/day of Risperdal
(depending on age) for at least 1 to 2 weeks, before introducing the
antidepressant drug. A smoother transition and response will be
observed, with significantly less risk of vicious paradoxical rage
behaviour.?
http://www.netrover.com/~southgve/druguse1.htm
?Risperdal (generic name: Risperidone):
Risperdal, like other new antipsychotic drugs currently under
development, is designed as a serotonin/dopamine antagonist. While its
exact mechanism of action is not yet understood, Risperdal seems to
block the action of serotonin and dopamine, two neurotransmitter
chemicals in the brain. Conventional antipsychotics seem to primarily
affect only dopamine.?
?Risperidone:
a drug used to treat problem behaviours such as aggression,
self-injury, and irritability in children, adolescents, and adults
with autism. The drug works by reducing abnormal excitement in the
brain.?
http://www.cairn-site.com/glossary/glossary.html#R
?The so-called atypical neuroleptics are recent discoveries. They
blend functionality against schizophrenia, psychosis, self-injurious
behavior, painful ticcing, and other major mental-health symptoms with
far fewer side effects and dangers than their ancestors. Patients
currently taking older neuroleptics should definitely ask their
physician about making a switch. The atypical neuroleptic family
includes:
? clozapine (Clozaril)
? olanzapine (Zyprexa)
? risperidone (Risperdal)
? quetiapine (Seroquel)
? ziprasidone (Zeldox)
Of these, risperidone and olanzapine have gotten the most attention
for their beneficial effects on some people with PDDs. The two are
similar in that they both target serotonin and dopamine receptors, but
there are subtle differences. Perhaps they each block different
receptors. Several recent studies have pronounced these two
medications to be reasonably effective for problems ranging from
Tourette Syndrome with rage attacks to severe autistic behaviors.?
http://www.patientcenters.com/autism/news/meds.html#neuroleptics
?Risperidone is a very strong dopamine blocker (antagonist); i.e., it
inhibits functioning of dopamine receptors.
It reaches peak plasma levels quickly regardless of whether it is
administered as a liquid or pills. The strong dopamine-blocking
reaction is known to make some people feel nauseated if they do things
that normally trigger the dopamine response, such as eat a pleasing
meal or experience orgasm. Risperidone is metabolised fairly quickly
so this potential for nausea subsides usually in two to three hours.?
http://www.reference.com/browse/wiki/Risperidone
?"The implications of this work may potentially extend beyond
Asperger's disorder," Dr. Rausch and colleagues write. "It is possible
that a number of negative symptom spectrum disorders may respond to
such treatment. It is also possible that some neurochemical processes
linked to negative symptoms in schizophrenia could be present in
Asperger's disorder, insofar as there may be some commonalities of
neuropharmacologic response."
http://healthlibrary.epnet.com/GetContent.aspx?token=712c416e-2228-4a57-ae0e-b2be76d615d5&chunkiid=104247
?How cortisol & cytokine imbalance may lead to autism
Cortisol and other glucocorticoids act on cells in the hippocampus,
dentate gyrus and elsewhere to facilitate planned apoptosis. In the
developing brain there are several ways in which cortisol and related
hormones can be prevented from reaching the developing brain.
Specifically, we identify prenatal factors including 1) placental
factors, 2) maternal cortisol binding proteins, 3) interference with
signal transmission in the developing brain, 4) abnormal levels of
cytokines and 5) possible maternal immune response to embryonic GnRH.
It may be that a failure of any one or all of these may lead to the
failure of apoptosis or misapoptosis. In the post-natal period the
infants adrenocortical, pituitary and hypothalamic factors become
important. The post natal developing brain still needs planned
apoptosis. Since the data on increased head circumference and
presumably the failure of apoptosis, cortisol and cytokines most
likely play a role here (Akshoomoff, et al 2002). Cortisol and
cytokines are responsible for: 1) facilitation of planned apoptosis,
2) to provide the careful balance of hormones in the brain and 3) to
protect against aberrant immune system responses.?
This site has oodles of information on the chemistry of autism.
Copyright restrictions prevent me from posting more here.
http://neurosciencealliance.com/_wsn/page2.html
http://www.rxlist.com/cgi/generic/risperid_cp.htm
?Secretion of prolactin by the pituitary is under inhibitory control
via dopamine from the hypothalamus. Interference with dopamine
secretion or action leads to an increase in serum prolactin. Some
medicines can do this by blocking dopamine's action on the pituitary
(e.g. phenothiazines, butyrophenones, metoclopramide, risperidone) or
by depleting dopamine (e.g. methyldopa, reserpine).1 Opiates can
stimulate prolactin release.2 Other causes of hyperprolactinaemia
include diseases of the pituitary (e.g. prolactin secreting pituitary
adenomas) or hypothalamus, severe primary hypothyroidism, liver
cirrhosis, end stage renal disease, stress, high dose oestrogens and
chronic cocaine use.1
Dopamine receptor dysfunction is thought to be part of the
pathophysiology of schizophrenia.3 There are four major dopaminergic
pathways (mesolimbic, mesocortical, nigrostriatal, tuberoinfundibular)
and five types of dopamine receptors (D1-5). D2 receptors are found in
all the pathways.
In addition, serotonin receptors are believed to play a role in
psychosis.3 Serotonin is a modulator of dopamine; if the 5HT2A
serotonin receptor is blocked, this leads to an increase in dopamine
concentration. The action of antipsychotics depends on their relative
affinities for receptors of dopamine and serotonin.
Typical antipsychotics, such as haloperidol, act by blocking D2
receptors in a non-specific fashion. This results in different effects
on the four dopaminergic pathways: in the limbic system, it decreases
positive psychotic symptoms; in the tuberoinfundibular system, it
causes hyperprolactinaemia; and in the nigrostriatal system, it can
result in extrapyramidal symptoms (EPS). The effects on the
mesocortical pathway are less clear, and may be a combination of
therapeutic benefits and drug-induced 'negative' symptoms.?
?Risperidone can cause sustained hyperprolactinaemia
In contrast to the other atypicals, treatment with risperidone can
result in a sustained elevated prolactin level. It causes a rapid5,
dose-dependent rise in prolactin3 similar to that observed with
haloperidol.6 However, an analysis of randomised double-blind studies
of risperidone found the level of prolactin did not correlate with the
incidence of clinically detected prolactin-related adverse effects in
either sex at usual doses.6 Sustained hyperprolactinaemia is less
frequent with the other atypicals.
Although olanzapine causes an early dose-related rise in prolactin,
this is less frequent and less marked than that seen with haloperidol,
and is usually transient.7 A rise in prolactin is seen in about half
of patients on olanzapine compared to over 90% of those taking
risperidone, and enduring increases were less frequent in those taking
olanzapine.8
Why the difference? Risperidone has a high affinity for D2 as well as
serotonin receptors.3 It is not "limbic specific" for the mesolimbic
over the nigrostriatal tract like the other atypicals.9 Risperidone
antagonises dopamine in the tuberoinfundibular system causing a rise
in prolactin. However, its antagonist action at 5HT,sub>2A receptors
in the nigrostriatal pathways may partially explain why risperidone
has a low propensity to cause EPS despite its blockade of D2
receptors.?
http://www.medsafe.govt.nz/Profs/PUarticles/hyperpro.htm
From PubMed:
?More risperidone-treated subjects (87%) showed global improvement in
their condition compared with the placebo group (40%). Somnolence, the
most frequently reported adverse event, was noted in 72.5% versus 7.7%
of subjects (risperidone vs placebo) and seemed manageable with
dose/dose-schedule modification. Risperidone-treated subjects
experienced statistically significantly greater increases in weight
(2.7 vs 1.0 kg), pulse rate, and systolic blood pressure.
Extrapyramidal symptoms scores were comparable between groups.
CONCLUSIONS: Risperidone was well tolerated and efficacious in
treating behavioral symptoms associated with PDD in children.?
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Abstract&list_uids=15492353
Read this site for further interesting information. Look for the lines that say:
receptor occupancy rates.
receptor occupancy rates
black and white rates chart
black and white rates chart
for charts that depict receptor occupancy rates.
http://www.chovil.com/second.html
?Attention-deficit/hyperactivity disorder
People affected by attention-deficit/hyperactivity disorder (ADHD)
experience difficulties in the areas of attention, overactivity,
impulse control, and distractibility. Research shows that dopamine and
norepinephrine imbalances are strongly implicated in causing ADHD.?
http://www.minddisorders.com/Kau-Nu/Neurotransmitters.html
Side Effects:
==============
?Interference With Cognitive and Motor Performance - Since RISPERDAL�
has the potential to impair judgment, thinking, or motor skills,
patients should be cautioned about operating hazardous machinery,
including automobiles, until they are reasonably certain that
RISPERDAL� therapy does not affect them adversely.?
http://redpoll.pharmacy.ualberta.ca/drugbank/drugBank/drugFile/pi/APRD00187.html
Illustrations:
===============
Neurotransmitters
http://www.minddisorders.com/images/gemd_02_img0071.jpg
http://www.colorado.edu/epob/epob3730rlynch/image/figure6-11.jpg
http://www.patientcenters.com/autism/graphics/pdd0103.gif
This chart illustrates the receptors that Resperidol acts on:
http://www.nature.com/npp/journal/v28/n2/images/1300057t1.gif
Finally, this site is somewhat of an Aspie portal with links to
support groups and further information,
http://www.reference.com/browse/wiki/Asperger%27s_syndrome
I hope this has helped you! If anything is unclear, please request an
Answer Clarification, and allow me to respond, before you rate. I will
be happy to assist you further, before you rate this answer.
I wish you the best of luck!
Sincerely, Crabcakes
Search Terms
=============
Risperidone + mechanism of action
Risperidone + + pharmokinetics
risperidone + aspergers
dopamine + serotonin + receptors + Risperidone
neuroleptics + Aspergers |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}