Hello Lipofred,
Love your screen name!
LDL (low density lipoprotein) and HDL(high density lipoprotein) are
protein-bound forms (lipoprotein) of cholesterol. The cholesterol
molecule binds with a protein in order to travel! The ?good?
cholesterol, HDL is believed to transport cholesterol back to the
liver, where it is metabolized and excreted.
This site has a great explanation of how LDL transports
cholesterol. (Please read the whole paragraph on lipids-this may be a
slow loading page for you)
?Cholesterol is a hydrophobic molecule and quite insoluble in water.
Thus it cannot pass from the liver and/or the intestine to the cells
simply dissolved in blood and ECF. Instead it is carried in tiny
droplets of lipoprotein. The most abundant cholesterol carriers in
humans are the low-density lipoproteins or LDLs.?
http://users.rcn.com/jkimball.ma.ultranet/BiologyPages/E/Endocytosis.html#ldl
?High-density lipoprotein (HDL) or ?Good Cholesterol? carries about
one-third to one-fourth of blood cholesterol. Experts think HDL tends
to carry cholesterol away from the arteries and back to the liver,
where it is metabolised and removed. It is believed that HDL can
remove excess cholesterol from plaques and therefore slow their
growth. However, while a high level of HDL decreases the associated
risks, a low level of HDL cholesterol level may increase the
possibility of stroke or heart attack?
?Low-density lipoprotein (LDL) or ?Bad Cholesterol? is the major
cholesterol carrier in the blood. If too much LDL cholesterol
circulates in the blood, it can slowly build up in the walls of the
arteries feeding the heart and brain. Together with other substances
it can form plaque, a thick, hard deposit that can clog those arteries
(a condition known as atherosclerosis). A clot (thrombus) forming near
this plaque can block the blood flow to part of the heart muscle
resulting in a heart attack or it can block the blood flow to part of
the brain, causing a stroke. ?
http://www.chm.bris.ac.uk/webprojects2003/hails/transport.htm
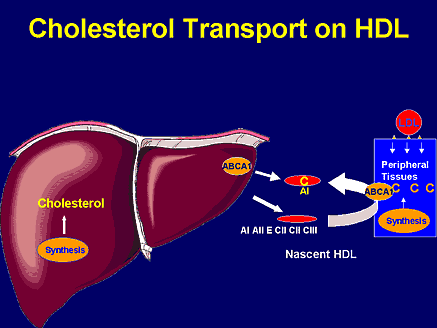
?The main task of HDL is to carry cholesterol from the peripheral
tissues, including the artery walls, to the liver. Here it is excreted
with the bile, or used for other purposes, for instance as a starting
point for the manufacture of important hormones. The LDL submarines
mainly transport cholesterol in the opposite direction. They carry it
from the liver, where most of our body's cholesterol is produced, to
the peripheral tissues, including the vascular walls. When cells need
cholesterol, they call for the LDL submarines, which then deliver
cholesterol into the interior of the cells. Most of the cholesterol in
the blood, between 60 and 80 per cent, is transported by LDL and is
called ?bad? cholesterol, for reasons that I shall explain soon. Only
15-20 percent is transported by HDL and called ?good? cholesterol. A
small part of the circulating cholesterol is transported by other
lipoproteins. ?
http://www.ravnskov.nu/myth1.htm
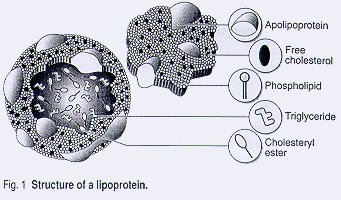
?Lipoproteins are complexes of lipids and proteins held together by
non-covalent bonds. Each type of lipoprotein has a characteristic
mass, chemical composition, density and physiological role.
Irrespective of density or particle size, circulating lipids consist
of a core of cholesteryl esters and triglycerides, an envelope of
phospholipids and free cholesterol and apolipoproteins. The
apolipoproteins are involved in the assembly and secretion of the
lipoprotein, provide structural integrity, activate
lipoprotein-modifying enzymes, and are the ligand for a large
assortment of receptors and membrane proteins.2 Each type of
lipoprotein has a characteristic apolipoprotein composition or ratio.
The most prominent apolipoprotein in HDL is apolipoprotein-AI
(apo-AI), which accounts for approximately 70% of the protein mass,
with apo-AII accounting for another 20%.2 The ratio of apoA-I to
apoA-II determines HDL functional and antiatherogenic properties.3
Circulating HDL particles consist of a hetergeneous mixture of
discoidal and spherical particles with a mass of 200 to 400
kilo-daltons and a diameter of 70 to 100 angstroms.2?
?Differences in the quantitative and qualitative content of lipids,
apolipoproteins, enzymes and lipid transfer proteins result in the
presence of various HDL subclasses, which are characterized by
differences in shape, density, size, charge and antigenicty.6 On the
basis of flotation rate in the preparative ultracentrifuge, there are
two major subclasses of HDL: HDL2 and HDL3.7 Due to the higher PAFAH
activity associated with HDL2, it has a greater oxidative protective
effect than HDL3. The difference in the distribution of antioxidants
between HDL2 and HDL3 also helps to explain the difference in their
anti-oxidative protective effect against LDL oxidation.8 HDL2
particles are depleted in cholesteryl ester and enriched in
triglycerides. Hepatic lipase acts on the large, triglyceride-rich
HDL2 to hydrolyze the triglycerides, converting HDL2 to HDL3. HDL3
then serves as an acceptor for free cholesterol, perpetuating the
HDL2-HDL3 cycle.9?
http://www.musc.edu/bmt737/spring2001/Andrea/index.htm
There is even another form of cholesterol, not as well known:
?What is Lp(a) cholesterol?
Lp(a) is a genetic variation of plasma LDL. A high level of Lp(a) is
an important risk factor for developing fatty deposits in arteries
prematurely. The way an increased Lp(a) contributes to disease isn?t
understood. The lesions in artery walls contain substances that may
interact with Lp(a), leading to the buildup of fatty deposits.?
http://www.americanheart.org/presenter.jhtml?identifier=180
?HDL-Cholesterol is a high density lipoprotein, which is commonly
referred to as the "good" cholesterol. HDL-Cholesterol is a transport
protein which carries cholesterol away from the vessel wall for
removal from the body. The higher the HDL value, the lower the risk of
coronary artery disease. Exercise and weight loss has been shown to
increase your HDL level, while smoking has been shown to decrease it.
LDL-Cholesterol is a low density lipoprotein, which is commonly
referred to as the "bad" cholesterol. LDL-Cholesterol, like
HDL-Cholesterol, is a transport protein, however LDL transports
cholesterol to the vessels. The lower the LDL-Cholesterol, the lower
the risk of coronary artery disease. A low-fat, low-cholesterol
nutrition plan has been shown to decrease this value.
VLDL Cholesterol is the bodies fat transportation mechanism. This
value is not clinically measured, but rather the triglycerides value
divided by five. Low values are not clinically significant.
Cholesterol/HDL Ratio is a ratio of total cholesterol to
HDL-cholesterol, or simply a ratio of bad cholesterol to good
cholesterol. This ratio has been shown to be a good predictor of
coronary risk, with the lower the ratio the better. A combination of
regular aerobic exercise and good nutritional practices has been shown
to improve this ratio.
LDL/HDL Ratio is a further breakdown of your ratio of LDL-cholesterol
to HDL-cholesterol, simply the cholesterol delivery mechanism divided
by the cholesterol removal mechanism.?
http://www.baysport.com/bloodexp.shtml
?Cholesterol is removed from the vessel wall and transported to the
liver through a process called reverse cholesterol transport. Nuclear
receptors are among the most important transcription factors
regulating genes involved in different steps of reverse cholesterol
transport. Here, we discuss the role of the nuclear receptors LXR
(liver X receptor) and HNF-4a (hepatocyte nuclear factor-4a) in
different steps of reverse cholesterol transport. LXR controls the
transcription of crucial genes in cholesterol efflux from macrophages
and its transport to the liver, such as ABCA1 (ATP binding cassette
A1), CYP27A1 (sterol 27-hydroxylase), CLA-1 (scavenger receptor type
B1) and apolipoprotein E. Some oxysterols present in oxidized
low-density lipoproteins and proinflammatory cytokines modulate the
activity of LXR by antagonizing the effect of activators of this
receptor, thus contributing to cholesterol accumulation in
macrophages. Bile acid synthesis, which represents the final step of
reverse cholesterol transport, is transcriptionally regulated by
several nuclear receptors at the level of the liver-specific
cytochrome P450 cholesterol 7a-hydroxylase (CYP7A1), the rate-limiting
enzyme of this metabolic pathway. Bile acids returning to the liver
through the enterohepatic circulation down-regulate CYP7A1
transcription via the bile acid sensors farnesoid X receptor and
HNF-4a. Based on this evidence, these nuclear receptors are candidate
targets of new drugs for the treatment and prevention of
atherosclerotic disease.?
http://www.biochemsoctrans.org/bst/032/0092/bst0320092.htm
Perhaps these illustrations will be useful:
http://www.cumc.columbia.edu/news/in-vivo/Vol1_Iss5_mar11_02/cholesterol.html
http://www.colorado.edu/MCDB/MCDB1150/ohd/ldl.jpg
http://160.114.99.91/astrojan/Prot/Ldl.jpg
http://www.biochemsoctrans.org/bst/032/0092/bst0320092f01.gif
http://images.medscape.com/pi/editorial/cmecircle/2003/2494/images/brown/slide19.gif
http://www.chm.bris.ac.uk/webprojects2003/hails/lipo1.jpg
I hope this has helped you! Please ask for an Answer Clarification,
before you rate, if anything is unclear.
Regards, Crabcakes
Search Terms
============
Lipid transport
HDL + LDL function |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}